
Department of Anesthesiology, Perioperative and Pain Medicine
Stanford University
California
CareArea Perioperative Care, Business Unit Therapy
Drägerwerk AG & Co. KGaA
Luebeck, Germany
Just like our automobiles, the anesthesia machines we use today are far more complex than the ones we used during our training. They have more electronic components, more valves, different gas flow pathways, and it can be more difficult to sort out what is going on under the hood when things go awry.

We present the case of a patient under anesthesia with a rising end-tidal carbon dioxide (ETCO2) level that was found to be caused by an obstructed soda lime canister. Since it has been reported that the patient’s other ventilation and vital sign parameters—such as oxygen saturation, tidal volume delivered, and peak and plateau airway pressures—remained normal, we review the background and reasons why this could have happened and examine how this problem might have been diagnosed before the induction of anesthesia.
Case Presentation
An otherwise healthy 40-year-old man (ASA physical status IE) presented for emergency release of a bowel obstruction. The anesthesia machine in the OR was an Apollo anesthesia workstation (Dräger). Prior to the case start, the anesthesia technician was observed replacing the disposable carbon dioxide (CO2) absorber in the correct fashion. The red cap over the absorber’s air inlet (Figure 1) had been removed as required before insertion. Before the induction of anesthesia, it has been reported that the anesthesia machine had passed both the Dräger automatic test and the American Society of Anesthesiologists-approved anesthesia apparatus checkout recommendation.1
Preoxygenation was performed per institutional routine with a mask held gently over the patient’s face. After an uneventful rapid sequence induction and intubation, mechanical ventilation commenced. The ETCO2 was noted to rise progressively over the next few minutes. It has been reported that no other changes were noted in the patient’s vital signs or the ventilation parameters. There was no tachycardia or any other sign to suggest malignant hyperthermia. Furthermore, no changes in oxygen saturation, airway pressure or tidal volume were reported. The machine was replaced with another anesthesia machine, and the ETCO2 returned to normal. The case concluded uneventfully and the patient recovered normally from the anesthetic.
Subsequent inspection of the first anesthesia machine revealed that the inlet for gases of the CO2 absorber (Dräger CLIC Absorber 800+) was occluded completely with transparent tape (Figure 2).

The root cause of the mishap was traced to a technician who had unpacked a box of absorber canisters and noticed that one of them was missing the red cap that should cover the gas inlet. The technician covered the inlet with transparent tape to prevent the soda lime in the canister from becoming contaminated or inactive. Another technician failed to notice the tape on the canister when he used it to replace an exhausted one.2
Discussion
We were at a loss initially to understand how an occlusion of the soda lime canister could cause no other changes in mechanical ventilation parameters and become obvious only by means of the rising ETCO2 level.
Initially, we thought, the answer must lie in the fact that the Apollo anesthesia machine is designed to be functional during controlled ventilation whether there is a soda lime canister in place or not. This feature allows the anesthesiologist to change an exhausted canister during mid-case without pausing ventilation. The CLIC absorber into which the CO2 canister is inserted has a ring seal that makes it airtight and a flap mechanism that is activated when the soda lime reservoir is unlocked, thus sealing off the machine and allowing mechanical ventilation to continue uninterrupted.3,4
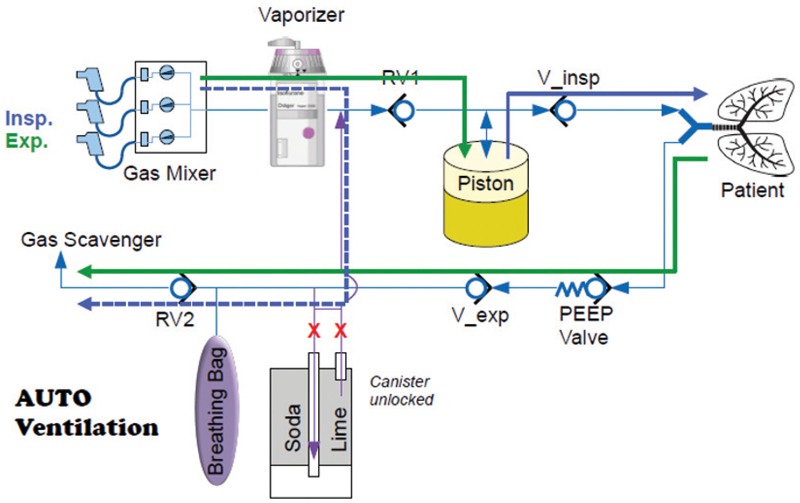
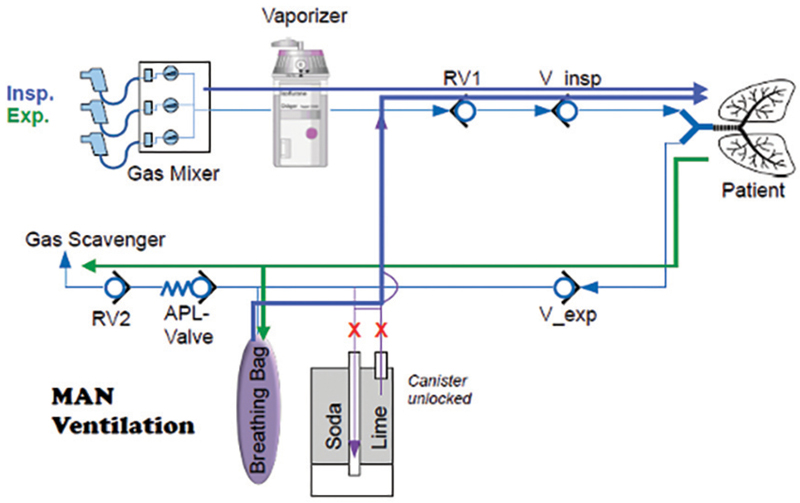
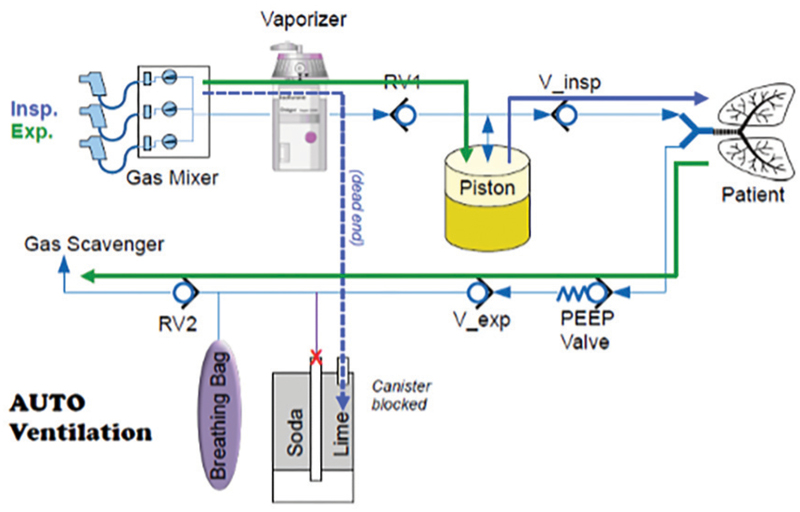
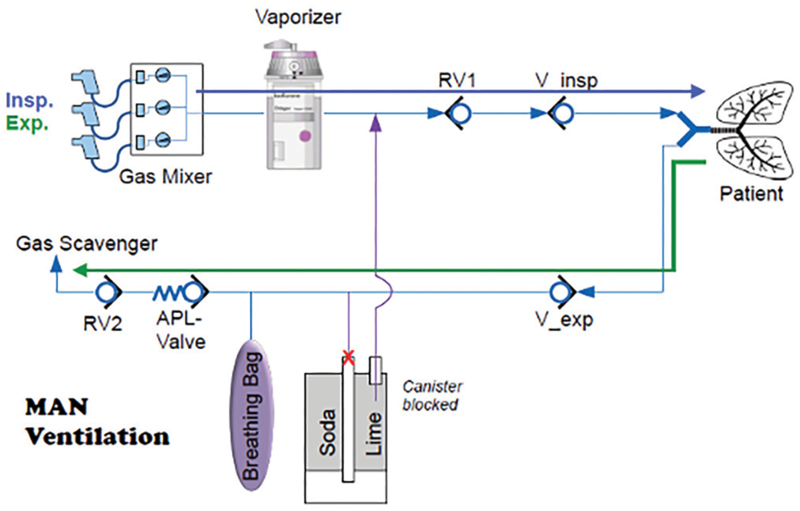
However, after review with the manufacturer, we recognized that the occluded CO2 absorber in our case creates a different situation from the “intended” unlocking mechanism of the CO2 absorber, which allows exchange of CO2 absorbent during the case. With an unlocked CO2 absorber, both manual ventilation and mechanical ventilation are possible since the CO2 absorber is simply “bypassed” (Figures 3 and 4). In our case, the CO2 absorber was blocked, which turned the circular system into an open system, with no rebreathing possibility, and therefore no possibility to either breathe spontaneously or perform manual ventilation (Figures 5 and 6).
Other case reports involving the CLIC absorber system have noted that controlled ventilation will proceed uneventfully even if there is a leak in the soda lime canister,5 or if the canister has not been properly inserted.6 However, manual ventilation with the reservoir bag in any of these scenarios will be difficult or impossible because it immediately reveals a large leak in the system. This is why it is important to repeat the leak test whenever the CO2 absorber is changed before a new case begins.
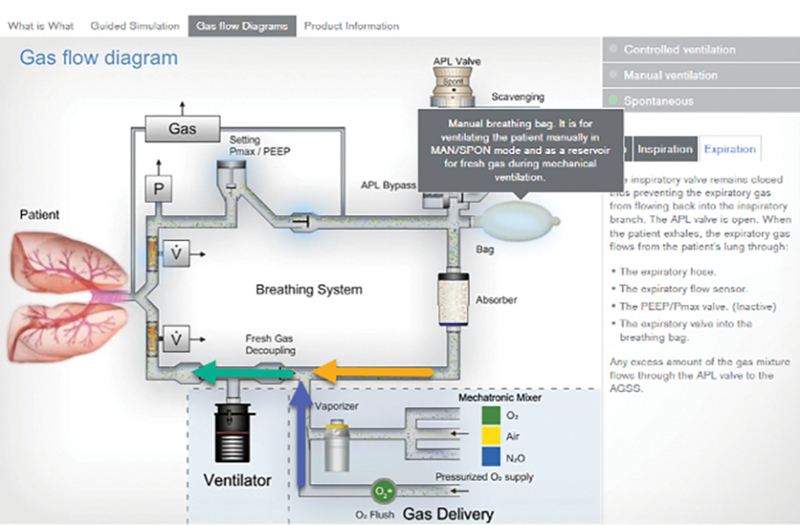
In the case of this patient, there was no leak and controlled ventilation was reported to be normal in all respects other than the rising ETCO2. This is because the inflow of gas in the Apollo machine during controlled ventilation does not need to pass through the soda lime canister. The fresh gas flow on inspiration proceeds directly through the inspiratory valve and sensor, through the Y-piece and into the patient’s lungs. (Please refer to the animated Dräger gas flow diagram for controlled ventilation.7) This means as long as the fresh gas flow is much higher than the minute ventilation of the patient, the ventilation of the patient would not be affected and such obstruction would not be apparent.

In contrast, if the fresh gas flow is lower than the minute ventilation, the piston would not receive enough fresh gas for applying the set ventilation volumes/pressures, thus leading to hypoventilation. The increasing ETCO2 was the clinical sign of hypoventilation. At the same time, Apollo gives an additional alarm message—“fresh gas low”—as soon as the Apollo recognizes that the delivered fresh gas flow is set too low to serve the required volume from the patient.
On expiration, the exhaled gas and gas mixture in the reservoir bag normally flow through the absorber where CO2 is removed from the gas mixture and the scrubbed gas reenters the inspiratory side of the breathing system. If the exhaled gas cannot pass through the CO2 canister due to obstruction, as in this case, then it simply is vented out through the scavenging system.
During spontaneous breathing, on the other hand, the flow of gas through the system is different. (Please refer to the animated Dräger gas flow diagram for spontaneous breathing.7) The patient inhales gas from both the reservoir bag and the fresh gas flow (Figure 7). The gas flows from the reservoir bag through the CO2 absorber, merges with the fresh gas flow, passes through the inspiratory valve and sensor, and then through the Y-piece and into the patient.6 Since the pressure source in manual ventilation is squeezing the bag, flow through the CO2 absorber from the reservoir bag is obligatory. This means that if the CO2 absorber is blocked (and not bypassed), there is no flow of gas possible to the patient.
We suspect that the problem was not revealed in our case during the preoxygenation process because the face mask was held gently rather than with a tight seal. This was done to reduce anxiety for the patient. However, it may have permitted some room air to be entrained, and thus apparently it concealed the obstruction of the breathing system by the occluded CO2 canister in manual ventilation mode with the breathing bag.
As a result, we undertook a volunteer study. We deliberately inserted an identical CO2 absorber with the inlet port covered with tape into an Apollo Anesthesia Workstation. This was done to document what would happen to a spontaneously breathing, unanesthetized subject during simulated preoxygenation with a tightly fitting face mask compared with a loosely fitted one.
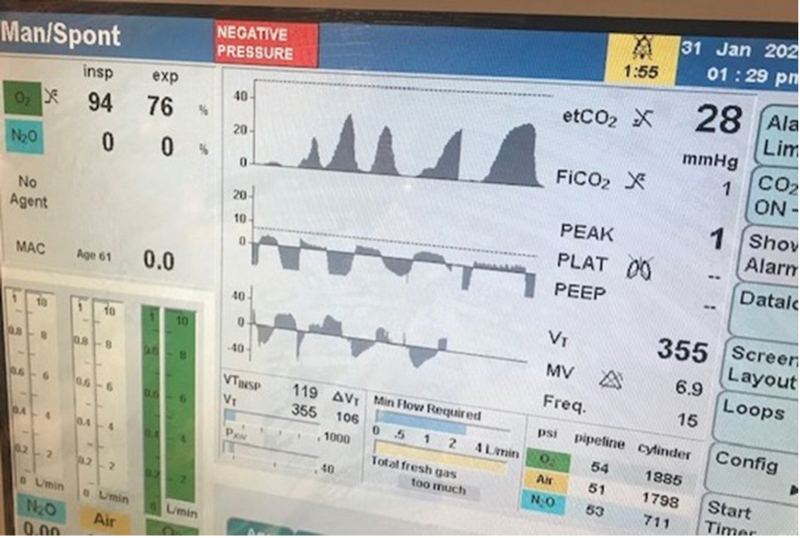
The result of this study was that when we placed a tightly fitting mask over the volunteer’s face with oxygen flowing at 10 L per minute, attempts to breathe became increasingly difficult, indicating obstruction of gas flow from the system. This was confirmed by the activation of the negative pressure alarm on the Apollo display screen (Figure 8). When the face mask was not held tightly and room air could be entrained, no breathing difficulty was detected.
It is important to remember also that pressure and leak testing will not necessarily identify obstruction within the breathing circuit. Testing should be done before each procedure to ensure that gas flows properly through the circuit during both inspiration and exhalation. This may be done by attaching a “test lung” or second reservoir bag to the patient end of the circuit, setting fresh gas flow at 5 L per minute, and manually squeezing the reservoir bag.8
Conclusion
- Technical staff must be adequately trained to look after anesthesia equipment safety. In this case, a technician’s good intentions paved the way for a system malfunction.
- If the system inflow to the CO2 absorber is blocked, preoxygenation can still proceed uneventfully as long as the face mask is applied loosely, and the problem will remain undetected. Once the patient is intubated, mechanical ventilation will be possible, but no exhaled gas will pass through the absorber. If the fresh gas flow is lower than the minute volume of the patient, the ETCO2 will continue to rise and the alarm “fresh gas low” will be triggered.
- It is important to check all parts of the manual pre-use check on any anesthesia machine before starting the automatic part of the self-test. In the case described, checking item 11 on the Apollo check list, “CO2 absorbent OK?” might have detected the occluded CO2. canister.
- It is important to follow the Anesthesia Patient Safety Foundation/ASA guidelines on proper machine check-out. In the case described, checking item 13, “Verify that gas flows properly through the breathing circuit during both inspiration and exhalation,” could also have detected the problem.9
- Preoxygenation with a tightly fitting face mask during spontaneous breathing could have enabled early diagnosis of the problem.
- One technician found a missing red cap on one of the absorbers. He replaced the red cap with a transparent, difficult-to-see tape. The color red of this cap represents a warning color. Modifying a medical device, by replacing a red warning mark with a transparent mark is a unapproved modification or unapproved mislabeling of a medical device. Such modifications are not allowed to be done.
- We hope that with this communication this problem will not happen to the reader. In conclusion, any unexpected high ETCO2 during anesthesia must be investigated. If a diagnosis can’t be made, then the anesthesia machine must be replaced, just like it was done in this case.
“The Frost Series” is named in recognition of Elizabeth Frost, MD, who started this feature in the early 1980s.
Sibert, a past president of the California Society of Anesthesiologists and member of the Anesthesiology News editorial advisory board, is the medical editor of “The Frost Series.” Authors who wish to submit a case to her may send it to FrostCaseSubmission@gmail.com. Please limit text to about 1,200 words and include an image, if possible.
References
- Brock-Utne JG. Case #77: technical staff must be well trained. In: Anesthesia in Low-Resourced Settings: Near Misses and Lessons Learned. 1st ed. Springer; 2021.
- Another reason for pre-oxygenation with a tight-fitted face mask. Presented at: the American Society of Anesthesiologists Annual Meeting; October 21-25, 2022; New Orleans, LA.
- Dräger. Just “CLIC” it! 2015. Accessed January 25, 2023. https://www.draeger.com/Content/Documents/Products/lsa_draegersorb_clic_casestudy_9051467_en.pdf
- Schüler HU, Goldbeck B, Karchner D. In response: a novel cause of rebreathing carbon dioxide related to removed CLIC-seal on the Dräger Apollo Anesthesia Machine. J Clin Monit Comput. 2019;33(2):353-355.
- Kuruma Y, Kita Y, Fujii S. Exchanging a CLIC absorber in the middle of surgery. APSF Newsletter. 2013;27(3).
- Pai S-L, Robards CB, Riutort KT, et al. Oxygen delivery failure due to improper installation of carbon dioxide absorbent canister: a case report. Braz J Anesthesiol. 2021;71(4):443-446.
- Dräger. Apollo gas flow diagrams for controlled ventilation and spontaneous breathing. 2010. Accessed January 25, 2024. https://anesthesia-products.azurewebsites.net/apollo/D1100
- Prien T, Brinker A, Pfeiffer K, et al. Equipment problems. Preventable anesthetic deaths: Is “PaF” the magic dragon? Anesth Analg. 2019;129(5):1439-1441.
- American Society of Anesthesiologists. 2008 ASA Recommendations for Pre Anesthesia Checkout | American Society of Anesthesiologists (ASA) (asahq.org). Accessed January 25, 2024.
- Pai S-L, Robards CB, Riutort KT, et al. Oxygen delivery failure due to improper installation of carbon dioxide absorbent canister: a case report. Braz J Anesthesiol. 2021;71(4):443-446.
- Dräger. Apollo gas flow diagrams for controlled ventilation and spontaneous breathing. 2010. Accessed January 25, 2024. https://anesthesia-products.azurewebsites.net/apollo/D1100
- Prien T, Brinker A, Pfeiffer K, et al. Equipment problems. Preventable anesthetic deaths: Is “PaF” the magic dragon? Anesth Analg. 2019;129(5):1439-1441.
- American Society of Anesthesiologists. 2008 ASA Recommendations for Pre Anesthesia Checkout | American Society of Anesthesiologists (ASA) (asahq.org). Accessed January 25, 2024.